Last week in Pulmonary Report, we talked about a case of isolated mediastinal/hilar adenopathy (IMHL). 4 important differential considerations were discussed:
Infection (esp. MTB)
Sarcoidosis
Malignancy (metastatic solid organ or lymphoma)
Reactive
We discussed several studies that evaluated the optimal evaluation for suspicious IMHL, as well as factors which were shown retrospectively to be suggestive of reactive adenopathy.
This week in Pulmonary Report, Dr. Ludwig presented the case of a 68 year old man with chronic exertional dyspnea and abnormal PFTs. Her evaluation (which is still ongoing!) tackled a a high-yield and challenging topic – what happens when your patient has restrictive PFTs but doesn’t have parenchymal disease to explain it?
The broad categories of restrictive lung disease can be remembered with the mnemonic PAINT:
In our patient’s case, an HRCT was performed and did not reveal clear parenchymal/pleural causes of restriction, leading us down the “extra-parenchymal” pathway:
Slide: extra-parenchymal causes of restrictive lung dz
Several maneuvers are available to aid in the differential diagnosis of a restrictive PFT
Supine and upright VC may suggest neuromuscular causes of restrictive lung disease.
Normal lung function – decrease of 3-8% from upright to supine
Significant diaphragm dysfunction – >15%
Chest wall and diaphragm mechanics
MVV (or maximal voluntary ventilation) wherein patients are asked to take rapid deep breaths for 12 seconds, is demonstrated in the video below:
MVVpred = FEV1 x ~35-40 (lower values suggestive of neuromuscular weakness)
Maximum inspiratory/expiratory pressure (MIP and MEP) are also decreased in neuromuscular disease:
Pre (upright) and post (supine) flow-volume loop
Pre (upright) and post (supine) vital capacity
MIP and MEP
Diaphragm function may also be evaluated using other modalities:
Diaphragm ultrasound for excursion and fractional thickening
Obtaining a diaphragmatic ultrasound
Thickening fraction: [(thickness at end-inspiration—thickness at end-expiration)/thickness at end-expiration]. <20% is indicative of diaphragmatic weakness
Normal diaphragm excursion: 6cm (female) 7cm (male) during deep breathing
Electromyography of diaphragm to assess for innervation
Using esophageal or surface electrodes below lower frontal/dorsal ribs
Negative conduction does not distinguish between neuropathic/myopathic causes and may be followed up with nerve stimulation test
Fluoroscopic sniff test can be used to detect unilateral pathology
Poor sensitivity in bilateral paralysis; accessory muscle use may cause upward displacement of ribs creating appearance of downward displacement of diaphragm
Sensitivity in unilateral paralysis is ~90%
Finally, some management considerations for respiratory symptoms in the patient with neuromuscular disease:
Consider blood gas testing for hypercapnia when FVC <40% pred
It’s been awhile since our last ILD round-up, but we are glad to be back in action! This week we talked about a young man with CVID, ITPand persistent groundglass opacities. We discussed a concern for granulomatous and lymphocytic interstitial lung disease (GL-ILD)
I. What is GL-ILD?
Seen in patients with CVID. With the advent of effective therapies (namely IVIG), increased prevalence of non-infectious complications of CVID (non-infectious complications now seen in 70% of patients with CVID).
GL-ILD is seen in 8-20% of cases of CVID, making it the most common ILD in this condition. It may also be seen in CTLA-4 deficiency. Associated with splenomegaly, immune-mediated cytopenias, and ITP. BAL demonstrates increased percentage of CD21lo B cells. Pathology demonstrates a peribronchiolar lymphocytic infiltrate, usually associated with granulomas (94% in one case series) and often with organization.
Image: peribronchial and interstitial lymphocytic infiltration
Image: Epithelioid granuloma
II. What are the characteristic HRCT findings of GL-ILD?
Solid & subsolid nodules, groundglass opacities, reticulations, mediastinal and hilar adenopathy. Less likely to contain reticulation, TBE, honeycombing, masses or consolidation. A radiologic DDX includes infection, organizing pneumonia, LIP, sarcoidosis and lymphoma. As alreadt noted, splenomegaly (bottom image) is common.
III. How is GL-ILD treated?
Consensus guidelines with strong agreement that mainstay of therapy is optimization of IVIG therapy. Whether to proactively treat or enter active surveillance after IVIG optimization is less well established, nor is whether antibiotic prophylaxis (as is often the case in CVID) is warranted. Corticosteroids are frequently used, but without clear evidence basis or consensus. Potential second line agents include azathioprine, rituximab, MMF.
Join us at 8:30 – Short Presentations – Session One – Baldwin Auditorium – as Dr. Rowe presents our preliminary data from the blog and highlights our experiences.
9:00 – Dr. Rowe will present at Eco-Normalization – Searle room
1:45 – Discussing Interactive Asynchronous Learning session – Baldwin Auditorium – a range of experiences with the modern digital age of medical education, including a piece about medical education blogging! Featuring also Dr. Angarone of our friend blog, bit.ly/nuidblog
We’re so glad you’re here, and are always excited to chat about our experience, hear your suggestions, or collaborate!
#NUPCCM Blog Team
Update – thanks to all who came out to support us, and for all of you visiting the blog for the first time after our presentation. We had a great time with the discussion and can’t wait to see the community continue to grow!
From left: Mike Angarone, Mac Walter, Brianna Valdes, Tim Rowe, Tricia Pendergrast
Thanks to Dr. Rowe for a great morning report case – a middle aged man with well-controlled HIV, ESRD on HD, referred to clinic for an abnormal CT as part of pre-transplant workup.
CT with some moderate subcarinal and right paratracheal lymphadenopathy, minimal parenchymal findings.
What next?
Differential:
Sarcoidosis
Infection (TB, endemic fungi, anything really)
Malignancy
Reactive
EBUS to the rescue! – REMEDY: AJRCCM 2012 study showed that EBUS mediastinoscopies in 87% of cases – 67/77 cases were diagnosed with EBUS; of the 10 undiagnosed, only 6 got diagnoses in mediastinoscopy
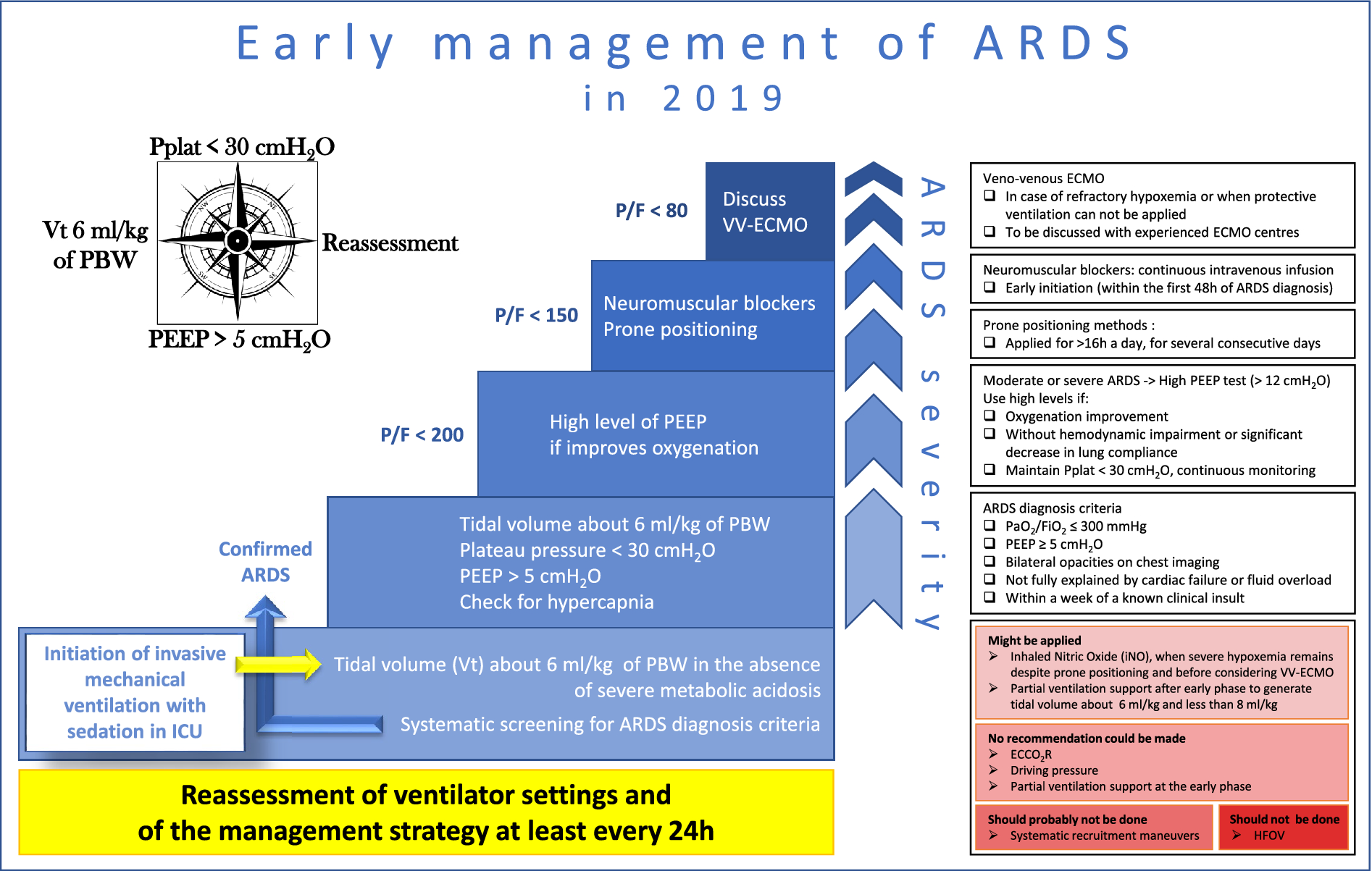
Consensus guidelines on use of NIV in respiratory failure. A nice summary of the literature on the use of NIV in the pre-intubation and post-extubation setting
Summary of 3 important guidelines from the ATS/ACCP on evidence-based liberation from mechanical ventilation in critically ill adults. References to the parent documents are provided in this summary
Retrospective analysis of PROSEVA data which found that did not find an association between the improvement in gas exchange and survival – suggesting perhaps that proning mechanism of benefit is largely through limiting VILI
Evidence-based multi-society guidelines on mechanical ventilation in ARDS. Only LTVV + Pplt < 30 cmH20 and prone positioning for > 12hrs/day in severe ARDS receive strong recommendations FOR
Question: Does aggressive fluid resuscitation compared to moderate fluid resuscitation improve clinical outcomes in patients with acute pancreatitis?
Why ask it: How to administer intravenous fluids (IVF) for patients with acute pancreatitis remains a source of debate. Early IVF may improve pancreatic microcirculatory hypoperfusion and help prevent pancreatic necrosis. However, excessive IVF can contribute to complications including respiratory failure and abdominal compartment syndrome.
Intervention: 249 patients in 8 countries presenting to the emergency department with mild acute pancreatitis randomized to aggressive or moderate fluid resuscitation protocols (see comment for important exclusion criteria and details of intervention).
Results (all written as aggressive IVF group vs moderate IVF group):
Development of moderately severe or severe acute pancreatitis (primary outcome)
The trial was halted by the DSMB at the first interim analysis due to worse safety outcomes in the aggressive IVF group
Similar results in prespecified subgroup analyses of patients with SIRS at baseline and those with baseline hypovolemia
Conclusion: In patients with mild acute pancreatitis, aggressive IVF did not improve clinical outcomes and was associated with more fluid overload compared to moderate IVF.
Comments:
Acute pancreatitis pathobiology
Intra-acinar activation of trypsin causes autodigestive injury to the vascular endothelium, interstitium, and acinar cells with a resulting inflammatory response
Acute pancreatitis and sepsis share similar pathobiology including microcirculatory dysfunction, dysregulated inflammatory and coagulation cascades, and the potential for systemic and end-organ complications
Central goals of IVF in acute pancreatitis are the correction of hypovolemia and restoration of perfusion to the pancreatic microcirculation
WATERFALL was a multi-center, open-label, parallel-group, controlled superiority trial conducted at 18 centers in 4 countries (India, Italy, Mexico, Spain)
Many exclusion criteria
Moderately severe or severe disease per the Revised Atlanta Classification
NYHA CHF II – IV
Uncontrolled HTN
Hyper or hyponatremia
Hyperkalemia
Hypercalcemia
Life expectancy < 1 year
Chronic pancreatitis
Chronic renal failure
Decompensated cirrhosis
Details of interventions (Lactated Ringers used for all)
Aggressive-resuscitation group
Enrollment
Bolus 20 mL/kg, then infusion 3 mL/kg/hr
Hour 3 (“safety checkpoint”)
Physical assessment to evaluate for signs of volume overload
If present, decrease or stop infusion
Hours 12, 24, 48, and 72 (“goal-directed therapy checkpoints”)
Hypovolemia
Bolus 20 mL/kg, then infusion 3mL/kg/hr
Additional boluses of 20 mL/kg if low UOP or SBP
Normovolemia
Infusion 1.5 mL/kg/hr
Stop after 48 hrs if oral feeding tolerated for > 8 hrs
Suspicion of fluid overload
Decrease or stop infusion
Infusion stopped after 48 hrs if oral feeding tolerated for > 8hr
Moderate-resuscitation group
Enrollment
1.5 mL/kg/hr without bolus in pts without hypovolemia
If hypovolemia present, bolus 10 ml/kg over 2 hrs then start infusion
Hour 3
Physical assessment to evaluate for signs of volume overload
If present, decrease or stop infusion
Hours 12, 24, 48, and 72
Hypovolemia
Bolus 10 mL/kg, then infusion 1.5 mL/kg/hr
Additional boluses of 10 ml/kg if low UOP or SBP
Normovolemia
Infusion 1.5 mL/kg/hr
Stop after 20 hrs if oral feeding tolerated for > 8 hrs
Suspicion of fluid overload
Decrease or stop infusion
Infusion stopped after 20 hrs if oral feeding tolerated for > 8hr
Oral feeding started at 12 hrs in both groups if minimal abd pain per the PAN-PROMISE SCORE
Fluid overload identified by at least 2 of the following: symptoms, physical signs, and imaging evidence of hypervolemia
Notable patient characteristics
Age: ~57
Gallstone pancreatitis: 61%
CAD: 1%
Median BiSPAP score: 1
2 or more SIRS: 26%
Results of intervention (all written as aggressive IVF group vs moderate IVF group)
The intensity of bedside reassessment in the trial (structured safety and goal-directed therapy checks at hours 3, 12, 24, 48, and 72) exceeds what is provided for many hospitalized patients in a real-world setting. The trial therefore likely underestimates the harm associated with aggressive IVF in less monitored settings.
By design, the patients in this trial were not that sick. They had minimal co-morbidities and they could not have any organ failures or local/systemic complications related to their acute pancreatitis at the time of enrollment. The results are therefore not generalizable to the care of critically ill patients with acute pancreatitis. Patients who present with severe disease (who may have more pronounced hypovolemia and be at higher risk of progression to necrotizing pancreatitis) may uniquely benefit from IVF. Conversely, those with chronic pulmonary, cardiac, and renal disease are at higher risk of developing clinically significant complications from aggressive IVF. A tough balance.
The trial aimed to enroll 744 patients to detect a 10% difference between groups in the development of moderately severe or severe acute pancreatitis assuming an incidence of 35%. Given the lower-than-expected incidence of moderately severe or severe acute pancreatitis during the trial (20% overall) and the early trial termination at an enrollment of 249 patients, the study is underpowered to detect differences in the primary outcome
This trial does not inform a safe lower limit for IVF in acute pancreatitis. Do patients really need an infusion of 1.5 mL/kg/hr at days 2 and 3? My guess is no but this trial doesn’t answer that.
My simplified view is that we should approach IVF resuscitation in acute pancreatitis much like we do with sepsis (they share many similarities as noted above). IVF in both settings is probably of most benefit when given early and in patients with more severe disease. For the floor patients we evaluate for MICU transfer (worsening disease or organ dysfunction several days into their hospital stay), ongoing high-volume maintenance fluids are likely of little benefit.
As in sepsis care, there is not one perfect marker to guide resuscitation in acute pancreatitis. IVF should be guided by serial reassessment of intravascular volume, perfusion pressure, and tissue oxygenation using all of the imperfect tools at our disposal rather than a one-size-fits-all protocol.
Thanks to Ale for sharing a case of a young man without any significant PMH who had chest pain and cough and abnormal imaging. Sent to ED with left upper lobe pneumothorax that improved with a small bore chest tube.
What’s the differential for spontaneous pneumothorax in this kind of case? What is the long-term management?
This week, a 75-year-old woman former smoker with history of recurrent PEs with abnormal CT imaging was presented. Her work up was notable for a +ANA (1:640) and an HP panel with low-level positive mold antibodies. A TTE showed normal LV and RV size and function with a mildly elevated RVSP. Her high-resolution chest CT had evidence of prominent mosaic attenuation, peripheral and peribronchovascular reticulations, ground glass, traction bronchiectasis, and extensive air trapping. Her PFTs normalized with a course of prednisone except for a persistent, mildly reduced DLCO. The patient had improvement in her cough and SOB but still had spells of lightheadedness. The question presented to the group was “Is there a need for further diagnostics for HP or pulmonary hypertension?”
I. What is mosaic attenuation?
Mosaic attenuation on CT is a heterogeneous pattern of attenuation that resembles…a mosaic.
Differential for mosaic attenuation secondary to small airways disease:
In this patient, the presence of mosaic attenuation could represent either HP, mosaic oligemia from pulmonary vascular disease, or both.
II. Is there a way to differentiate between etiologies of mosaic attenuation radiologically?
As mentioned by Dr Rishi Agrawal, one of the best ways to distinguish small airways disease from other forms of mosaic attenuation is by looking at your expiratory imaging on HRCT.
In non-airways-related causes of mosaic attenuation, the lungs should increase in attenuation on expiratory imaging diffusely. This contrasts with what you should see in small-airways disease, where gas trapping will accentuate differences in attenuation.
III. Takeaways
Mosaic attenuation is a non-specific finding on CT that can represent disease of the small airways, interstitium, alveoli, or pulmonary vasculature.
In an undifferentiated patient, it is important to consider mosaic oligemia 2/2 PAH as a cause of mosaic attenuation.
Pulmonary diseases affecting the small airways includes a broad differential (table above for reference).
If the attenuation diffusely increases on expiration, it suggests that the etiology of the mosaic attenuation is NOT related to the small airways.
References:
Fleischner Society: Glossary of Terms for Thoracic Imaging https://doi-org.turing.library.northwestern.edu/10.1148/radiol.2462070712
Mosaic Attenuation: Etiology, Methods of Differentiation, and Pitfalls https://doi.org/10.1148/rg.2015140308














 Join us at 8:30 – Short Presentations – Session One – Baldwin Auditorium – as Dr. Rowe presents our preliminary data from the blog and highlights our experiences.
Join us at 8:30 – Short Presentations – Session One – Baldwin Auditorium – as Dr. Rowe presents our preliminary data from the blog and highlights our experiences.