
Thanks to third-year Ale for hosting us at her rooftop patio!

Thanks to third-year Ale for hosting us at her rooftop patio!


Some highlights about chylothorax from Amy’s great morning report case.

Chylothorax (picture from StatPearls:https://www.ncbi.nlm.nih.gov/books/NBK459206/)

Sources:
Amy Ludwig’s Morning Report


Congratulations to the PCCM Fellowship Class of 2022!





Thanks to Justin Fiala for these awesome 3D printed lung planters!

I tried to find data on alcohol based hand rubs in C.diff but all I found is that hand washing is recommended – see this small study of volunteers who had C.diff spores spread on their hands then either soap or alcohol, then shook hands with other volunteers – hand washing was better at removing spore counts – https://pubmed.ncbi.nlm.nih.gov/20429659
Surprisingly, the IDSA guidelines – https://www.idsociety.org/practice-guideline/clostridium-difficile/– say okay to do alcohol based cleaning if gloves are worn in routine and non-endemic settings, though acknowledges that handwashing with soap and water is superior to alcohol based hand hygiene
My practice will be to continue hand-washing after C.diff rooms, time-consuming as it is, because don’t want to bring it home to your cat or dog (happened to one of my residents; https://www.hcplive.com/view/potential-transfer-of-clostridium-difficile-from-dog-cat-to-household-owners)
Lots of activity on Twitter on CCR22 during the current Critical Care Review Meeting – #CCR22
I read a little more about the blood culture biofire that we’ve started seeing – BCID2 – 43 PCR results including organisms and resistance – https://www.biofiredx.com/products/the-filmarray-panels/filmarraybcid/ and some evidence – Banerjee et al randomized 617 patients with positive blood cultures to usual care (takes about two days to get results from micro lab cultures) vs BCID +- stewardship team – showed shorter time to organism identification and appropriate abx changes – no difference in mortality, LOS, or cost
![Comparison of time to organism identification, availability of phenotypic antimicrobial susceptibility results, and first appropriate modification of antimicrobial therapy for the subset of study subjects with organisms represented on the rapid multiplex polymerase chain reaction (rmPCR) panel (n = 481). Time 0 is when the positive Gram stain result was reported. Median time in hours (interquartile range [IQR]) to organism identification: control 22.3 (17–28), both rmPCR and rmPCR + stewardship 1.3 (0.9–1.6); de-escalation: control 39 (19–56), rmPCR 36 (22–61), rmPCR + stewardship 20 (6–36); escalation: control 18 (2–63), rmPCR 4 (1.5–24), rmPCR + stewardship 4 (1.8–9). *P < .05 vs control; †P < .05 vs control and rmPCR groups.](https://oup.silverchair-cdn.com/oup/backfile/Content_public/Journal/cid/61/7/10.1093_cid_civ447/1/m_civ44702.gif?Expires=1656615705&Signature=uh-Nv-ujh61U-Py8oZJa68o69fm10gzyNUYaLXd1MxR0febizhFFF97Xh0gMd3mJ3O-blQAJWKhQ~homJFlHMDgT~hft2KzOz1qmWvBDIsLg3LHtNh8pFE~zJ3vm6~lztWgAu3ixAcmqWV-esiEevvNG3glObWz2LXRXmV-4X3qSSySR-1VdqvVXpHkxeaOgN1v0N8Sm0KKqnHb65ifX8yK5UxYVmmrkSNdbyzWyi4IgLmAiulXeu5Xdvtq6jK3wbwsd2E0AD5wIQbUNkAc7Xf-s6fZ9P5iMdguVOFYPVyWaLL5kWPsLadiQEUEs2KmrerbW6nOd~Ofvbx38C4mDmg__&Key-Pair-Id=APKAIE5G5CRDK6RD3PGA) https://academic.oup.com/cid/article/61/7/1071/289120 They also have a small number of discrepancies (11 cases) in their Table 2 – but pretty reasonable and only 3 true cases of organism identification discrepancy
https://academic.oup.com/cid/article/61/7/1071/289120 They also have a small number of discrepancies (11 cases) in their Table 2 – but pretty reasonable and only 3 true cases of organism identification discrepancy
I’m excited to see this and look forward to using it clinically!
Iron is needed by bacteria
Higher iron associated with higher mortality in ICU patients – https://www.nature.com/articles/s41598-018-29353-2
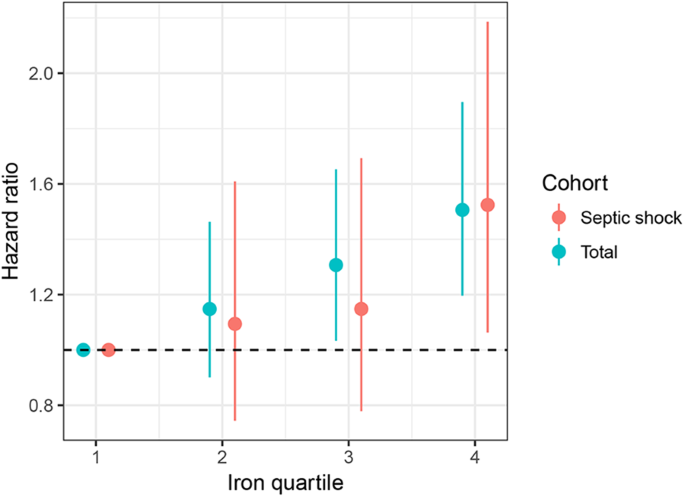
Animal sepsis models – giving iron in septic animals leads to increased mortality – https://pubmed.ncbi.nlm.nih.gov/15190970/
Giving IV iron to stable outpatients doesn’t necessarily increase infections – https://pubmed.ncbi.nlm.nih.gov/31485910/
But wouldn’t give it to septic patients (though note the data for this are sparse – https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3226152/)
 In fact, check out Cefiderocol – trojan horse antibiotic – two cephalosporins (ceftaz, cefepime) and catechol-type siderophore ~iron – gets taken up by bacteria but then attacked by antimicrobial! – https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7054475/ – just recently approved
In fact, check out Cefiderocol – trojan horse antibiotic – two cephalosporins (ceftaz, cefepime) and catechol-type siderophore ~iron – gets taken up by bacteria but then attacked by antimicrobial! – https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7054475/ – just recently approved

DEXA-ARDS study – Villar et al. in Lancet Resp –
https://www.thelancet.com/pdfs/journals/lanres/PIIS2213-2600(19)30417-5.pdf
https://www.thelancet.com/pdfs/journals/lanres/PIIS2213-2600(19)30417-5.pdf
RCT of 277 patients with ARDS P/F<200 todexa 20 daily x 5d then down to 10mg x5d or extubation; improved outcomes vent-free days, mortality (21% vs 36% at 60 days)! Rich says every few years steroids for ARDS come back into vogue but then another study shows no benefit or harm and the cyclerepeats though.

Pulmcrit has a nice summary of the previous studies too of steroids in ARDS – https://emcrit.org/pulmcrit/dexa-ards/
Wang et al. Accuracy of Ultrasound Jugular Venous Pressure Height in Predicting Central Venous Congestion. Annals of Internal Medicine. 2022
Question: Does ultrasound assessment of jugular venous pressure height (uJVP) in the semi-upright and upright positions predict elevated right atrial pressure (RAP) measured during right heart catheterization (RHC)?
Why ask it: Visual inspection of the height of the JVP is often used to estimate RAP. Patient anatomy and variation in the distance between the sternal angle and right atrium may limit the accuracy of this measurement. While ultrasound assessment of inferior vena cava (IVC) diameter and collapsibility is commonly used to estimate RAP, there are many patient and operator-specific limitations to this technique.
Intervention: Convenience sample of 100 patients undergoing RHC at the University of Utah. Two POCUS-trained cardiology fellows and 1 attending physician obtained the following values using a handheld ultrasound (Butterfly Network):
1. Quantitative uJVP: measured with HOB at 30-45° and defined as the point at which the internal jugular (IJ) vein tapered to smaller than the adjacent carotid artery throughout the respiratory cycle (vertical height of this taper above sternal angle + 5 cm = uJVP).
2. Qualitative uJVP based on neck zone where the IJ collapse point was identified: zone 1 (below clavicle), zone 2 (lower 3rd of neck), zone 3 (middle 3rd of neck), zone 4 (upper 3rd of neck), and zone 5 (above mandible).
3. Qualitative uJVP with HOB 90°: If IJ distended to at least the size of the adjacent carotid artery, this test was considered positive
Results:
Conclusion: Point-of-care ultrasound assessment of JVP can identify patients with an elevated RAP on RHC with a reasonable degree of accuracy
Comment:

